doi: 10.56294/saludcyt2024.918
ORIGINAL
Epidemiological study on Covid-19 frequency, severity, and territorial spreading
Estudio epidemiológico sobre la frecuencia, la gravedad y la extensión territorial del Covid-19
Nesamani Sonja J1 ![]() *, Charisma S. Ututalum2
*, Charisma S. Ututalum2 ![]() *, Prabakaran S3
*, Prabakaran S3 ![]() *, Himanshu Makhija4
*, Himanshu Makhija4 ![]() *,
Pooja Srishti5
*,
Pooja Srishti5 ![]() *, Prathima Prakasam6
*, Prathima Prakasam6 ![]() *
*
1College of Nursing, Aligarh Muslim University, Department of OBG Nursing. Aligarh, India.
2Sulu State College, Department of Nursing, Philippines.
3Sri Balaji Vidyapeeth (deemed to be university), Department of Pediatrics, Pondicherry, India.
4Chitkara University, Centre of Research Impact and Outcome, Punjab, India.
5Noida International University, Department of Allied Health Sciences, Greater Noida, India.
6Sree Vidyanikethan College of Nursing, Department of OBG, Andhra Pradesh, India.
Cite as: Sonja J N, Ututalum CS, S P, Makhija H, Srishti P, Prakasam P. Epidemiological study on Covid-19 frequency, severity, and territorial spreading. Salud, Ciencia y Tecnología. 2024; 4:.918. https://doi.org/10.56294/saludcyt2024.918
Submitted: 25-12-2023 Revised: 04-04-2024 Accepted: 26-08-2024 Published: 27-08-2024
Editor: Dr.
William Castillo-González ![]()
ABSTRACT
This study analyzes the descriptive epidemiology and testing performance in India has been thoroughly analyzed, revealing a robust and effective approach to reporting and managing COVID-19 cases. COVID-19 scenario reports from January 22, 2020 and April 30, 2020 in India. This research examines COVID-19 incidence, severity and spread. The examination frequency was explained spatially and temporally. Along with public health metrics and events, we showed trends and characterized instances by period location and individuals. During January 22, 2020 and April 30, 2020, people were tested for SARS-CoV-2; 40 184 (3,9 %) of the tests produced positive findings in India. Age-specific assault rates were lowest among children under 10 and highest among those aged 50-69. Positive instances were more common in encounters with complaints and in non-responsive people than in patients with SARI, overseas travel experiences or healthcare professionals. Males had a greater assault rate (41,64 %) over females (24,32 %). Six percent of attacks were secondary. In all, 71,1 % of 736 districts reported COVID-19 instances and 99 % percent of districts confirmed treatment.
Keywords: COVID-19; Infectious Disease; Epidemiology; Corona Virus and Novel Corona Virus.
RESUMEN
Este estudio analiza la epidemiología descriptiva y el rendimiento de las pruebas en la India se ha analizado a fondo, revelando un enfoque sólido y eficaz para informar y gestionar los casos de COVID-19. Se informa del escenario de COVID-19 entre el 22 de enero de 2020 y el 30 de abril de 2020 en la India. Esta investigación examina la incidencia, gravedad y propagación de COVID-19. La frecuencia de los exámenes se explicó espacial y temporalmente. Junto con métricas de salud pública y eventos, mostramos tendencias y caracterizamos instancias por ubicación de período e individuos. Durante el 22 de enero de 2020 y el 30 de abril de 2020, se realizaron pruebas a personas para detectar el SARS-CoV-2; 40 184 (3,9 %) de las pruebas dieron resultados positivos en la India. Las tasas de agresiones específicas por edad fueron más bajas entre los menores de 10 años y más altas entre las personas de 50 a 69 años. Los casos positivos fueron más frecuentes en encuentros con quejas y en personas que no respondían que en pacientes con SARI, experiencias de viajes al extranjero o profesionales sanitarios. Los varones presentaron una mayor tasa de agresiones (41,64 %) que las mujeres (24,32 %). El 6 % de las agresiones fueron secundarias. En total, el 71,1 % de los 736 distritos notificaron casos de COVID-19 y el 99 % de los distritos confirmaron el tratamiento.
Palabras clave: COVID-19; Enfermedad Infecciosa; Epidemiología; Virus Corona y Nuevo Virus Corona.
INTRODUCTION
The epidemic cause by the original corona virus SARS-CoV-2(1) has spread hastily across the globe, affecting many countries and resulting in exponential cases in some areas. The virus has caused a significant impact on public health, economies, and social structures, leading to widespread disruption of daily life for many individuals. While significant progress has been made in developing effective treatments and vaccines, the pandemic continues to threaten public health, particularly in areas with low vaccination rates or high transmission rates (2) of new variants of the virus. To ensure consistent validation of research findings (3), it is important to use rigorous methodologies that are transparent and reproducible. The clinical appearance of COVID-19 symptoms can embrace fever, tiredness, dehydrated cough, depression and breathing difficulty. Conversely, it is significant to note that the symptom of COVID-19 (4) knows how to differ between persons and some individuals may experience no symptoms at all. Certain things however, could become sick. In areas with limited healthcare resources, individuals may be less likely to receive timely and effective treatment for COVID-19, leading to higher rates (5) of severe illness and mortality. The holder fatality rate is designed by isolating the number of deaths by the integer of definite cases of COVID-19. A number of variables, including the inhabitants’ ages and medical conditions, the accessibility as well as the caliber of medical care (6) along with the period and efficacy of healthcare initiatives, could affect it. Numerous pathogen- and host-related variables may be connected to such significant individual variations in reaction to SARS-CoV-2(7) disease.
It converts enzyme 2 (ACE2) receptor DNA and modification alleles, the various compulsory affinities of angiotensin converting enzyme2 to the bug point (S) proteins (8) specified by its S and L subtypes, and the resulting degree of hyperactive cytokines is brought by innate immunity. Global attempts are being made to restrict the spread of the global disease (9), despite the fact that vaccinations are currently produced and being disseminated. The COVID-19 characterization in fourteen hospital staff members of individuals further strengthened the evidence of between people (10) transmission. Suggested that the virus could be transmitted from an infected person to another person through close contact, such as in a healthcare setting. This study examines the descriptive epidemiology and testing outcomes in India in detail, demonstrating a reliable and efficient method for reporting and handling COVID-19 cases. Statistical methods to examine data from a large number of patients suffering with severe COVID-19 (11) sickness, it is possible to determine which laboratory, demographic and quantitative characteristics are most significantly linked to death. Ongoing investigate is required to better appreciate the force of COVID-19 (12) on children and to develop appropriate prevention and treatment strategies. A multi-scalar technique was used on Portugal’s mainland to capture the relationship connecting change in movement patterns over the occasion and the related COVID-19 occurrence. The early outbreak phase of this epidemic may see super-spreading episodes (13), as it has been seen with other newly emerging viruses. However, it is unknown if this happened. Here, they examine 208 SARS-CoV-2 genome sequences that are accessible to the public gathered in the untimely stages of the scourge. The primary demographic differences affect how COVID-19 spreads and impacts populations (14), paying particular attention to the combined effects of period and masculinity as well as regional variations where resident’s density and dimension are input factor in the disease spreads along with the impact of disease morbidity and transience. This information enhances and complements epidemiological knowledge regarding the virus’s spread (15). A group of HLA alleles A, B, and C, identified as important in the immunological reaction to infection, corresponds with COVID-19 using an ecological method. The nationwide social defense division gave data for COVID-19(16), while information on HLA allele incidence was obtained from the Italians Bone Quintessence Donors Registry. The severe illness (17), linked to mortality, whichis documented in elderly and immune-compromised people with a history of other diseases. A multicenter trial involved 536 age-matched non-cancer participants and 105 cancer patients with verified COVID-19 status. The findings indicated that COVID-19 cancer patients had greater chances for all serious outcomes. Patients with metastatic, lung, or hematologic cancer (18) experienced the most severe effects. To aid in diagnosing and assessing the present epidemic in clinical decision-making, a Meta study was carried out to examine the effects of times, gender, comorbidities and clinical features on the brutality (19) of COVID-19. Identify nation with a high risk of unhygienic visitors as well as a tool for track pandemic’s development in a variety of nation. The ability of the practice to correspond to the entire dynamics (20) is controlled by the huge amount of COVID-19 cases that go unreported or demonstrate no symptom.
METHOD
Examinations of Frequency, Severity, and Territorial Spreading
COVID-19, caused by SARS-CoV-2, is a serious respiratory illness that, since its discovery at the end of the year 2019, has spread quickly over the world, affecting various aspects of health and global health.
Frequency: COVID-19 has caused over 5,7 million deaths and 408 million confirmed cases globally as of April 18, 2021. Despite vaccination efforts, global vaccine distribution and uptake remain unequal, affecting some countries.
Severity: COVID-19 presents mild to severe symptoms like fever, cough, and breathing difficulty, with severity varying based on age, health issues, and healthcare availability, making older individuals more susceptible.
Territorial spreading: COVID-19 has spread globally, spreading through respiratory droplets and contact with the face. Countries have implemented measures like social separation, mask mandates, and lockdowns to slow its spread, but these have significant social and economic impacts.
Experiments Performed using Certain Features are Described as Follows
The diagnostic features of a disease were assessed using the frequency of sample collection, number of tests, and test positives. The seven-day daily average was used to track positivity patterns, while the state-specific demographic median was used to calculate the average number of tests per million. Dividing the entire amount of tests across the cases decreased the chance of a case.
Cases by Location, Period, and Individual: An Analytical Epidemiology
The study used age, gender, place of residence, exposure, and symptoms to analyze case features. Population numerators determined the assault rate, and the percentage of secondary attacks among acquaintances was calculated.
RESULTS
SARS-CoV-2 testing was done on 1 021 518 individuals between January 22, 2020, and April 30, 2020. By the end of April 2020, the number of people tested and climbed around 250 daily in the initial stages of March 50 000 per day (table 1). Eight weeks later, there was a 200-fold rise in respiratory and nasal rinse assessments was observed, with 95 % of samples collected on the same day. Testing was conducted on 770 persons per million people, with states and Union Territories having the highest test frequency prevalence.
|
Table 1. District-level COVID-19 monitoring and frequency of evaluation |
||||
|
State/Union Territory |
Reporting regions |
Impacted areas |
Diagnostics per million people |
COVID-19 instances |
|
West Bengal |
23 |
20 |
402 |
1 155 |
|
Uttarakhand |
13 |
6 |
634 |
46 |
|
Uttar Pradesh |
75 |
66 |
343 |
2 175 |
|
Tripura |
8 |
3 |
1 251 |
3 |
|
Telangana |
33 |
29 |
475 |
941 |
|
Tamil Nadu |
38 |
36 |
1 468 |
2 108 |
|
Sikkim |
4 |
0 |
189 |
0 |
|
Rajasthan |
33 |
29 |
1 329 |
2 402 |
|
Punjab |
22 |
22 |
715 |
623 |
|
Puducherry |
4 |
2 |
2 092 |
8 |
|
Odisha |
30 |
16 |
646 |
172 |
|
Nagaland |
9 |
1 |
234 |
1 |
|
Mizoram |
7 |
1 |
172 |
1 |
|
Meghalaya |
11 |
2 |
488 |
11 |
|
Manipur |
14 |
2 |
182 |
2 |
|
Maharashtra |
36 |
36 |
1 070 |
14 305 |
|
Madhya Pradesh |
55 |
38 |
523 |
2 605 |
|
Lakshadweep |
1 |
0 |
5 136 |
0 |
|
Ladakh |
1 |
2 |
8 786 |
55 |
|
Kerala |
14 |
14 |
814 491 |
|
|
Karnataka |
30 |
23 |
1 011 |
535 |
|
Jharkhand |
24 |
12 |
285 |
113 |
|
Jammu and Kashmir |
20 |
16 |
1 417 |
685 |
|
Himachal Pradesh |
12 |
7 |
889 |
41 |
|
Haryana |
22 |
21 |
1 308 |
501 |
|
Gujarat |
33 |
30 |
1 133 |
4 694 |
|
Goa |
2 |
2 |
865 |
7 |
|
Delhi |
11 |
11 |
2 149 |
4 017 |
|
Daman and Diu |
2,1 |
0 |
3 588 |
0 |
|
Dadra and Nagar Haveli |
1 |
0 |
6 743 |
0 |
|
Chhattisgarh |
28 |
8 |
547 |
43 |
|
Chandigarh |
1 |
1 |
697 |
83 |
|
Bihar |
38 |
32 |
255 |
483 |
|
Assam |
32 |
19 |
228 |
94 |
|
Arunachal Pradesh |
25 |
1 |
499 |
1 |
|
Andhra Pradesh |
13 |
12 |
1 721 |
1 474 |
|
Andaman and Nicobar Islands |
3,2 |
3,1 |
5 423 |
40 |
|
Data not available |
_ |
_ |
_ |
269 |
|
India |
729 |
523 |
770 |
40 184 |
Indicative foreign visitors throughout the previous 14 days; B- Medical professionals with symptoms; C- individuals with SARI hospitalized; D- Healthcare personnel who are undiagnosed in contact with a verified case but lack adequate safeguards; E- Hot zones show the presence of ILI; F- Unspecified. Table 2 and figure 1 provide a comprehensive list of confirmed Cov-19 cases, including overall cases, total cases, and screening classifications, evaluated based on various criteria.
|
Table 2. Overview of COVID-19 tested individuals |
|||
|
Diagnostic classification |
Number of cases (%) |
Number tested (%) |
Positive (%) |
|
A |
1,3 |
1,7 |
3 |
|
B |
2,4 |
2 |
4,6 |
|
C |
10,5 |
6,8 |
6,1 |
|
D |
2,8 |
6,8 |
2,3 |
|
E |
3 |
4,8 |
2,6 |
|
F |
44,2 |
4,4 |
3,1 |
Figure 1. Diagnostic classification
The study discovered that individuals with severe acute respiratory infections (SARI) (6,1 %) and symptomatic contacts (10,3 %) had the greatest positive rates. The most common symptoms among 12 810 patients were fever and cough, with inability to breathe and sore throats observed in almost one-third of cases. Less than 5 % of cases showed digestive system symptoms, such as vomiting, diarrhea, nausea, and abdominal discomfort. Table 3 shows the symptoms of gathering specimen.
|
Table 3. Symptoms mentioned at the time of gathering specimen |
|
|
Symptom |
Total Number of Symptoms (%) |
|
Myalgia |
12,54 |
|
Abdominal Pain |
2 |
|
Symptomatic Without Details |
0,03 |
|
Sore Throat |
26,73 |
|
Vomiting |
4,39 |
|
Cough |
64,52 |
|
Expectoration |
5,45 |
|
Loose Stools |
3,17 |
|
Nausea |
2,54 |
|
Chest Pain |
0,1 |
|
Hemoptysis |
1,2 |
|
Fever |
60 |
|
Rhinorrhea |
4,82 |
|
Breathlessness |
31,9 |
The age groups of 50–59 and 60–69 had the greatest attack rates per million people, with the lowest rate among those under 10 years old and the highest among those aged 50-59 and 60-69. Men had a higher assault rate, with slightly higher positive test percentages are depicted in table 4 and figure 2.
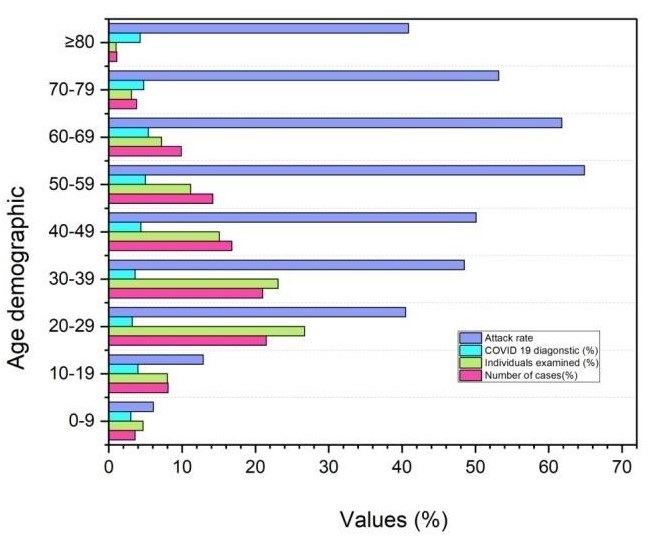
Figure 2. Age distribution
|
Table 4. Age demographics in the context of attack rate and case counts |
||||
|
Features |
Number of cases (%) |
Individuals examined (%) |
COVID-19 diagnostic (%) |
Attack rate |
|
Demography |
||||
|
0-9 |
3,61 |
4,72 |
3 |
6,11 |
|
10-19 |
8,13 |
8 |
4 |
12,93 |
|
20-29 |
21,54 |
26,74 |
3,22 |
40,51 |
|
30-39 |
21 |
23,13 |
3,64 |
48,52 |
|
40-49 |
16,83 |
15,11 |
4,43 |
50,13 |
|
50-59 |
14,21 |
11,23 |
5 |
64,91 |
|
60-69 |
9,94 |
7,24 |
5,41 |
61,84 |
|
70-79 |
3,83 |
3,12 |
4,82 |
53,21 |
|
≥80 |
1,11 |
1,04 |
4,31 |
40,94 |
|
Gender |
||||
|
Male |
64,52 |
67 |
3,83 |
41,64 |
|
Female |
35,54 |
33 |
4,24 |
24,32 |
|
Not included |
10 |
429 |
|
|
|
Aggregate |
40 184 |
1 021 518 |
3,91 |
33,23 |
DISCUSSION
The results showing heightened awareness and routine testing for SARS-CoV-2 infection, has put a Cov-19 laboratory-monitoring program in place. The majority of COVID instances in India were believed to be between intimate acquaintances, disproportionately affecting males and pensioners. The pandemic’s geographical distribution and stage have influenced the national testing plan, with evaluation sites gradually being deployed. Testing frequency and reimbursement have increased, but delays in sample collection highlight the rapidity of testing. Communication tracking is crucial for tracking the spread of infections among unrelated individuals. The ICMR’s SARS-CoV-2 program has made testing more accessible, but the increasing case rate has moderated. It recommends continuous examination, location monitoring, population evaluation, and operative studies.
CONCLUSIONS
SARS-CoV-2 testing on 1 021 518 individuals showed significant progress, with 40 000 positive results out of a total of 50 000 daily samples by April 2020, indicating a significant increase in testing volume. Incidence rates were greatest in symptoms and uninformed acquaintances, exceeding rates among patients with SARI illness, those who had been abroad before, and medical professionals. In terms of age, the assault rate (per million) was lowest (6,1 %) for those under 10 years old and highest (63,3 %) for those between the ages of 50 and 69. The assault rate was greater in males (41,64 %) than females (24,32 %). It was determined that the incidence of secondary attacks was 6,0 %. Remarkably, 736 districts confirmed testing in 99,0 % of them, and 71,1 % of them reported COVID-19 instances. Over time, the ICMR SARS-CoV-2 program has become more comprehensive and consistent. COVID-19 cases are widespread, with men and elderly individuals experiencing higher infection rates, especially with close companions. Data suggests the need for more monitoring strategies.
REFERENCES
1. Meskina, Elena R. “Preliminary clinical and epidemiological analysis of the first 1,000 pediatric COVID-19 cases in Moscow Region.” Journal of microbiology, epidemiology and immunobiology 97.3 (2020): 202-213.
2. Goujon, Anne, et al. “Demographic and territorial characteristics of COVID-19 cases and excess mortality in the European Union during the first wave.” Journal of Population Research 39.4 (2022): 533-556.
3. Pranzo, Andrea Marco Raffaele, Elena Dai Prà, and Angelo Besana. “Epidemiological geography at work: An exploratory review about the overall findings of spatial analysis applied to the study of CoViD-19 propagation along the first pandemic year.” GeoJournal 88.1 (2023): 1103-1125.
4. Reuben, Rine Christopher, et al. “Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria.” Journal of community health 46.3 (2021): 457-470.
5. Padhi, Sunali, et al. “ABO blood group system is associated with COVID-19 mortality: An epidemiological investigation in the Indian population.” Transfusion Clinique Et Biologique 27.4 (2020): 253-258.
6. Kishore, Kamal, et al. “Exploring the utility of Google mobility data during the COVID-19 pandemic in India: digital epidemiological analysis.” JMIR public health and surveillance 7.8 (2021): e29957.
7. Ahmed, Md Zahir, et al. “Epidemic of COVID-19 in China and associated psychological problems.” Asian journal of psychiatry 51 (2020): 102092.
8. Badawi, Alaa. “Hypercytokinemia and pathogen–host interaction in COVID-19.” Journal of Inflammation Research (2020): 255-261.
9. Dai, Mengyuan, et al. “Patients with cancer appear more vulnerable to SARS-CoV-2: a multicenter study during the COVID-19 outbreak.” Cancer discovery 10.6 (2020): 783-791.
10. Dhama, Kuldeep, et al. “An update on SARS-CoV-2/COVID-19 with particular reference to its clinical pathology, pathogenesis, immunopathology and mitigation strategies.” Travel medicine and infectious disease 37 (2020): 101755.
11. Hu, Chuanyu, et al. “Early prediction of mortality risk among patients with severe COVID-19, using machine learning.” International journal of epidemiology 49.6 (2020): 1918-1929.
12. Mileu, Nelson, et al. “Mobility and dissemination of COVID-19 in Portugal: correlations and estimates from Google’s mobility data.” Data 7.8 (2022): 107.
13. Wang, Liang, et al. “Inference of person-to-person transmission of COVID-19 reveals hidden super-spreading events during the early outbreak phase.” Nature communications 11.1 (2020): 5006.
14. Azzolina, Daniela, et al. “Gender and age factors affecting the mortality during the COVID-19 epidemic in Italy [Effetti del genere e dell’età sugli eccessi di mortalità durante l’epidemia di COVID-19 in Italia].” Epidemiologia e prevenzione 44.5-6 (2020): 252-259.
15. Correale, Pierpaolo, et al. “HLA-B* 44 and C* 01 prevalence correlates with Covid19 spreading across Italy.” International journal of molecular sciences 21.15 (2020): 5205.
16. Akbari, Ali, et al. “Early epidemiological analysis of CoVID-19: first report from South of Iran.” (2020).
17. Dai, Mengyuan, et al. “Patients with cancer appear more vulnerable to SARS-CoV-2: a multicenter study during the COVID-19 outbreak.” Cancer discovery 10.6 (2020): 783-791.
18. Barek, Md Abdul, Md Abdul Aziz, and Mohammad Safiqul Islam. “Impact of age, sex, comorbidities and clinical symptoms on the severity of COVID-19 cases: A meta-analysis with 55 studies and 10014 cases.” Heliyon 6.12 (2020).
19. Sominsky, Luba, David W. Walker, and Sarah J. Spencer. “One size does not fit all–Patterns of vulnerability and resilience in the COVID-19 pandemic and why heterogeneity of disease matters.” Brain, behavior, and immunity 87 (2020): 1.
20. Alteri, Claudia, et al. “Genomic epidemiology of SARS-CoV-2 reveals multiple lineages and early spread of SARS-CoV-2 infections in Lombardy, Italy.” Nature communications 12.1 (2021): 434.
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Data curation: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Formal analysis: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Research: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Methodology: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Resources: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Software: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Supervision: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Validation: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Drafting - original draft: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.
Writing - proofreading and editing: Nesamani Sonja J, Charisma S. Ututalum, Prabakaran S, Himanshu Makhija, Pooja Srishti, Prathima Prakasam.