ORIGINAL
Health-related quality of life in hypertensive regular basic education teachers who attend a Cardiology Clinic in North Lima
Calidad de vida relacionada con la salud en docentes hipertensos de educación básica regular que acuden a una Clínica de Cardiología de Lima Norte
Carlos La Rosa-Longobardi1 ![]() *, Lucia Asencios-Trujillo1
*, Lucia Asencios-Trujillo1 ![]() *, Lida Asencios-Trujillo1
*, Lida Asencios-Trujillo1 ![]() *, Djamila Gallegos-Espinoza1
*, Djamila Gallegos-Espinoza1 ![]() *, Livia Piñas-Rivera1
*, Livia Piñas-Rivera1 ![]() *, Hernan Matta- Solis2
*, Hernan Matta- Solis2 ![]() *
*
1Universidad Nacional de Educación Enrique Guzmán y Valle, Escuela de Posgrado. Lima, Perú.
2Instituto Peruano de Salud Familiar, TIC Research Center: eHealth & eEducation. Lima, Perú.
Cite as: Rosa-Longobardi CL, Asencios-Trujillo L, Asencios-Trujillo L, Gallegos-Espinoza D, Piñas-Rivera L, Solis HM-. Calidad de vida relacionada con la salud en docentes hipertensos de educación básica regular que acuden a una Clínica de Cardiología de Lima Norte. Salud, Ciencia y Tecnología 2024;4:736. https://doi.org/10.56294/saludcyt2024736.
Submitted: 07-10-2023 Revised: 27-12-2023 Accepted: 11-02-2024 Published: 12-02-2024
Editor: Dr.
William Castillo-González ![]()
ABSTRACT
Introduction: the Health-related quality of life considerably influences the well-being of the person, although when a disease occurs, this well-being tends to decrease and that this modifies the lifestyle of the person, therefore, the objective of the study is to determine the Health-related quality of life in relation to health in hypertensive regular basic education teachers who come to a cardiology clinic in North Lima, Methods: it is a quantitative, descriptive-cross-sectional study, with a total population of 124 hypertensive regular basic education teachers,
Results: in their results, we can observe that 13,7 % (n=17) have a very low Health-related quality of life in relation to their health, 26,6 % (n=33) low Health-related quality of life, 9,7 % (n=12) average Health-related quality of life, 43,5 % (n=54) high Health-related quality of life and 6,5 %(n=8) very high Health-related quality of life,
Conclusions: in conclusion, evaluations should be carried out in the health of the population, for the detection of risk factors and hypertension in an early stage.
Keywords: Health-related Quality of Life; Hypertension; Cardiovascular Risk.
RESUMEN
Introducción: La calidad de vida relacionada con la salud influye considerablemente en el bienestar de la persona, aunque cuando se presenta una enfermedad, este bienestar tiende a disminuir y que esto modifique el estilo de vida de la persona, por lo tanto, el objetivo del estudio es determinar la calidad de vida relacionada con la salud en relación a la salud en profesores de educación básica regular hipertensos que acuden a una clínica cardiológica de Lima Norte
Métodos: Es un estudio cuantitativo, descriptivo-transversal, con una población total de 124 profesores de educación básica regular hipertensos
Resultados: En sus resultados se observa que el 13,7 % (n=17) tienen una calidad de vida relacionada con la salud muy baja en relación a su salud, 26,6 % (n=33) calidad de vida relacionada con la salud baja, 9,7 % (n=12) calidad de vida relacionada con la salud media, 43,5 % (n=54) calidad de vida relacionada con la salud alta y 6,5 %(n=8) calidad de vida relacionada con la salud muy alta
Conclusiones: En conclusión, se deben realizar evaluaciones en la salud de la población, para la detección de factores de riesgo e hipertensión en etapa temprana.
Palabras clave: Calidad de Vida Relacionada con la Salud; Hipertensión; Riesgo Cardiovascular.
INTRODUCTION
The World Health Organization (WHO) reported that, per year, more than 15 million individuals are reported to die from NCDs (mostly 30 to 69 years of age), these deaths being mostly premature, which could be avoided; this phenomenon occurs mainly in countries with low to medium economies. Inadequate nutrition, intake of harmful substances and sedentary lifestyle condition people to suffer from more NCDs(1)
Hypertension (HTN) is the key risk factor for cardiovascular disability and death that impacts a high number of individuals globally. Particularly in low- and middle-economy countries such as China, Brazil, India and Mexico, where the economic burden of LCA and HT together contribute to 50 % of the total number of economic estimates identified(2)
In Latin American countries, the prevalence of hypertension is high, with the countries with the highest prevalence being Brazil with 25-35 %, Paraguay with 34 %, Chile with 33,7 %, Uruguay and Venezuela with 33 %; also, in Colombia by 25 %(3) It is estimated that, by 2025, the figure could increase to 60 % reaching a figure of 1 560 000 000 individuals globally(4)
Health-related quality of life (HRQOL) is a concept commonly used in the subjective assessment of a patient's health that reflects the patient's physical, psychological, social and emotional well-being as it is closely related to Health-related quality of life (QoL) and can cause an impact on their health status.(5,6)
However, hypertension negatively affects patient QoL especially in older people, who have more health care needs and are more likely to have worse HRQOL than healthy people(7,8)
For hypertensive patients, risk factors originate in two ways, the non-modifiable ones that are age, sex and genetics, which are aspects that are already established in humans; on the other hand, there are modifiable ones related to the habits and behaviors adopted in the lifestyle, the 12 which are food, the consumption of harmful substances and sedentary lifestyle(9,10)
Therefore, improving lifestyle, making healthy habits, adequate adherence to treatment and maintaining positive mental health will allow hypertensive patients to avoid or reduce risk factors that may have consequences on their health well-being(11,12)
In a study conducted in Poland, with participants between the ages of 30 to 89 years, they stated in their results that, the Health-related quality of life of people who were mostly men had a medium and good Health-related quality of life, concluding that healthy behaviors, follow the treatment properly and periodically take their blood pressure, towards keeping people's Health-related quality of life healthy(13)
In a study conducted in Pakistan, with 384 hypertensive participants, they observed in their results that, most of the participants were male, 56 % of them had a poor Health-related quality of life related to health between the ages of 41 to 50 years, concluding that by not making healthy habits for the management of their disease, tended to have an inadequate Health-related quality of life(14)
In a study carried out in Angola, with 113 participants, they stated in their results that, with respect to hypertensive participants, 64,6 % of them had a regular Health-related quality of life and 35,4 % a poor Health-related quality of life, concluding that the conditions and difficulty in accessing health services aggravate the disease due to factors such as overcrowding, inadequate feeding and poor living conditions(15)
Therefore, the research objective is to determine the health-related quality of life in relation to health in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima.
As justification, this research is very relevant for various reasons, whether hypertension is a chronic condition that affects the entire population, but that, in teachers, being exposed to stress factors and constant work, allows the risk that their quality of life is not adequate, since it influences their work performance and well-being.
METHODS
Research type and Design
In the study, according to its properties is quantitative, with respect to its methodology is descriptive-cross-sectional non-experimental.(16)
Population
The total population was made up of 192 people diagnosed with hypertension who attended the cardiology service of a health facility.
According to the study, the survey was conducted with a voluntary response sampling bias of the residents of the district since the type of sampling in the research was for convenience.
Inclusion Criteria
· People with hypertension over18 years old
· People with hypertension who are continuators in the cardiology service.
· People with hypertension who are within the authority of the healthcare facility.
· People who volunteer in the study
Technique and Instrument
The technique for the study is the survey, which was conducted using the questionnaire or data collection instrument Health-related quality of life Related to Health (SF-36).
The SF-36 is an instrument that is composed of 36 items distributed in 9 dimensions (physical functioning, physical role, body pain, general health, energy / fatigue, social functioning, emotional function, emotional well-being, and health change. In which its design is on a Likert-type scale, in which its scores range from 0 to 100 points, where, the response alternatives are varied, both polytomous and dichotomous and the higher the score, the higher the Health-related quality of life in relation to health hypertensive regular basic education teachers will have(17,18)
The sample adequacy measure to obtain the validation of the instrument by the Kaiser-Mayer-Olkin test obtained a coefficient of 0,901 (KMO > 0,8) and the Bartlett sphericity test obtained significant results (Approx. X2 = 6010,317; gl = 630; sig.= 0,000).
Finally, Cronbach's alpha internal consistency coefficient was 0,827 (α > 0,8; N of elements = 36), so it is determined that the instrument has a high degree of reliability.
Place and Application of the Instrument
It was coordinated in the first to coordinate the administrative procedures so that access to the health establishment is allowed and likewise to the users for the standard, in addition to providing information about the research and thus have the knowledge about what is going to be done.
RESULTS
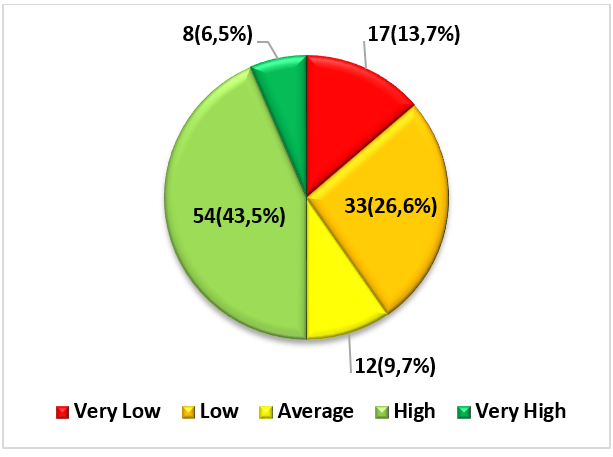
Figure 1. Health-related quality of life in relation to health in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 1, it can be seen that 13,7 % of participants have a very low Health-related quality of life in relation to their health, 26,6 % low Health-related quality of life, 9,7 % average Health-related quality of life, 43,5 % high Health-related quality of life and 6,5 % very high Health-related quality of life.

Figure 2. Health-related quality of life in relation to health in its physical functioning dimension in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 2, it could be observed with respect to the physical functioning dimension that, in their results, 25,8 % of the participants have a very low Health-related quality of life in relation to their health, 3,2 % low Health-related quality of life, 19,4 % average Health-related quality of life, 21 % high Health-related quality of life, 30,6 % very high Health-related quality of life.

Figure 3. Health-related quality of life in relation to health in its physical role dimension in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 3, with respect to the results of the physical role dimension, it can be seen that 40,3 % of the participants have a very low Health-related quality of life in relation to their health, 3,2 % average Health-related quality of life, 14,5 % high Health-related quality of life and 41,9 % very high Health-related quality of life.
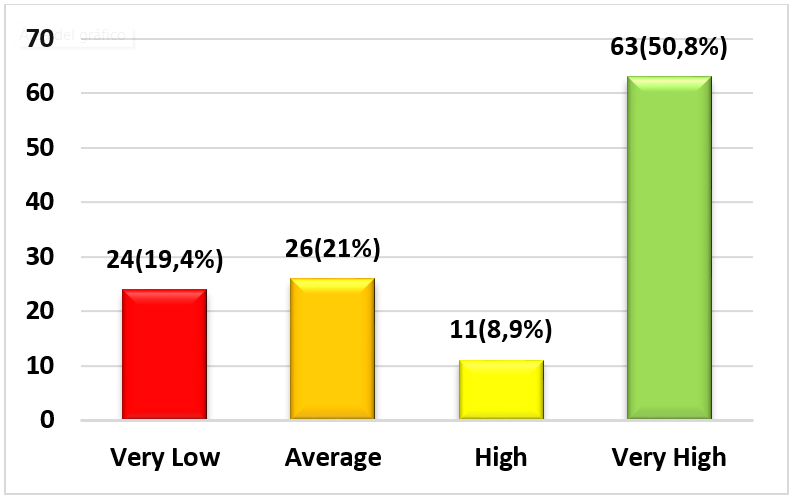
Figure 4. Health-related quality of life in relation to health in its dimension body pain in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 4, in the results of the body pain dimension, we can observe that 19,4 % of the participants have a very low Health-related quality of life in relation to their health, 21 % average Health-related quality of life, 8,9 % high Health-related quality of life and 50,8 % very high Health-related quality of life.
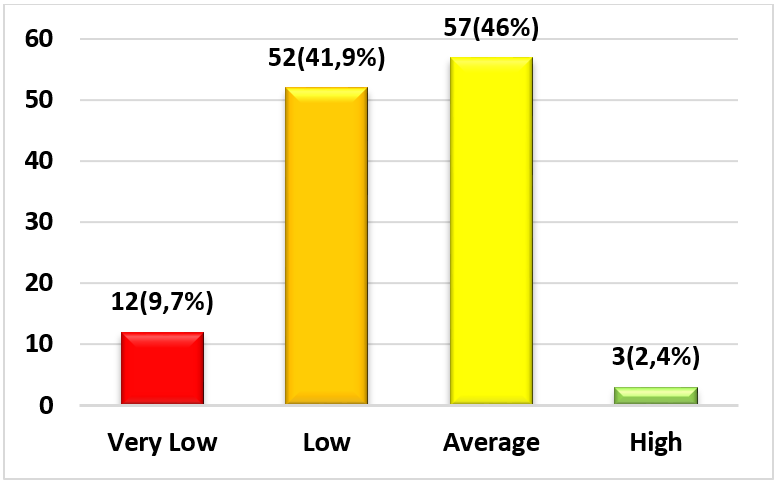
Figure 5. Health-related quality of life in relation to health in its general health dimension in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 5, with respect to the results of the general health dimension, it can be seen that 9,7 % of the participants have a very low Health-related quality of life in relation to their health, 41,9 % low Health-related quality of life, 46 % average Health-related quality of life and 2,4 % high Health-related quality of life.

Figure 6. Health-related quality of life in relation to health in its energy/fatigue dimension in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 6, with respect to the results of the energy/fatigue dimension, we can see that 3,2 % of the participants have a very low Health-related quality of life in relation to their health, 27,4 % low Health-related quality of life, 48,4 % average Health-related quality of life, 9,7 % high Health-related quality of life and 11,3 % very high Health-related quality of life.

Figure 7. Health-related quality of life in relation to health in its dimension social function in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 7, with respect to the results of the social function dimension, we can observe that 16,9 % of the participants have a very low Health-related quality of life in relation to their health, 24,2 % low Health-related quality of life, 13,7 % average Health-related quality of life, 35,5 % high Health-related quality of life and 9,7 % very high Health-related quality of life.

Figure 8. Health-related quality of life in relation to health in its dimension emotional function in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 8, we can observe with respect to the emotional function dimension that, 40,3 % of the participants have a very low Health-related quality of life in relation to their health, 4 % low Health-related quality of life, 12,1 % high Health-related quality of life, 43,5 % very high Health-related quality of life.

Figure 9. Health-related quality of life in relation to health in its dimension emotional well-being in hypertensive regular basic education teachers who attend a cardiology clinic in North Lima
In figure 9, with respect to the results of the emotional well-being dimension, we can observe that 0,8 % of the participants have a very low Health-related quality of life in relation to their health, 34,7 % low Health-related quality of life, 24,2 % average Health-related quality of life and 40,3 % high Health-related quality of life.

Figure 10. Health-related quality of life in relation to health in its dimension change of health in hypertensive regular basic education teachers who come to a cardiology clinic in North Lima
In figure 10, with respect to the results of the health change dimension, we can see that 21,8 % of the participants have a very low Health-related quality of life in relation to their health, 29,8 % average Health-related quality of life, 43,5 % high Health-related quality of life and 4,8 % very high Health-related quality of life.
DISCUSSION
NCDs and hypertension are health problems that are becoming increasingly frequent globally and in our country; The new ways of life, the advertising industry and the little impact obtained in education and health promotion, condition the health of today's individuals.
As for HRQOL, it presented a high level, this is because the health condition of hypertensive patients will depend on health controls, control of systolic BP, weight and the practice of lifestyles such as exercise and diet; especially in older adults who are more vulnerable to changes that may alter hypertension in their body and that can cause cardiovascular risks in the same affected their Health-related quality of life, therefore health education has a positive-significant impact on the knowledge, behaviors and HRQOL of hypertensive regular basic education teachers.
Regarding the dimension physical functioning and physical role, in their results it was observed that they presented a very low level of Health-related quality of life in relation to health, this is because they are closely linked and can be affected or not depending on the health condition, which in turn depends on the controls that the patient takes and the risk factors present. The older you are more likely to have comorbidities; Likewise, if systolic BP levels are not controlled, negative sequelae may appear that can severely affect the development of home and work activities. Older age and certain comorbidities affect the locomotor system, which limits physical activity related to domestic and work activities.
Regarding the other dimensions, we observed that, in their results they present average, high and very high levels, this is because, insufficient knowledge about hypertension and its care could lead to a less optimal control of systolic BP, which may be reflected in lower rates of adherence to prescribed antihypertensive medications and commitment to healthy lifestyle practices. The management of the pathology determines the condition and perception that one will have of their health that has been shown to promote an adequate control of BP and avoid the complications resulting from high BP. It is important to note that adherence to recommended antihypertensive medications is critical for proper disease control in addition to the practice of healthy lifestyles, resulting in reduced cardiovascular morbidity and mortality and lower health care costs.
Physical health when adequate is accompanied by vitality, this being an important aspect for the execution of daily activities. The vitality of hypertensive patients depends on their health condition. Improper management of the disease can lead to physical and emotional fatigue.
Patient education is essential to have optimal results in these hypertensive patients. If they are aware of their illness, they will be able to contribute more to their own care and self-care. The control of systolic BP and feeding should be emphasized. The health professional should inquire about the risk factors that impact the health of these patients, mainly modifiable ones, an effective management of these contributes to a better evolution and results of HRQOL.
That is why this research can develop different strategies for practice and policy to improve the quality of life in teachers with hypertension, strategies such as medical practice and comprehensive care, labor welfare programs, health and education policies among others that help this.
CONCLUSIONS
In conclusion, health activities in the population must be realigned in an integral way, in which it allows educating the population on how to improve the health-related quality of life.
It is concluded that evaluations should be conducted in the health of the population, for the detection of risk factors and hypertension at an early stage.
It is concluded that preventive strategies should be provided to help raise awareness of the population with hypertension that allows them to conduct their adequate controls for their disease, so that they have good health and general well-being.
The limitation in our study is that some hypertensive teachers being in this condition did not attend their controls, which did not allow the same day to fill out the survey, and had to be done on other days, but that, in addition to access to them to be in the study that mostly accepted.
REFERENCES
1. Organización Mundial de la Salud. Noncommunicable diseases Key facts People at risk Risk factors. OMS 2022. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
2. Zhang Q, Huang F, Zhang L, Li S, Zhang J. The effect of high blood pressure-health literacy, self-management behavior, self-efficacy and social support on the health-related quality of life of Kazakh hypertension patients in a low-income rural area of China: a structural equation model. BMC Public Health 2021;21:1–10. https://doi.org/10.1186/s12889-021-11129-5.
3. Barradas S, Lucumi D, Agudelo D, Mentz G. Socioeconomic position and quality of life among Colombian hypertensive patients: The mediating effect of perceived stress. Health Psychology Open 2021;8:1–9. https://doi.org/10.1177/2055102921996934.
4. Siddique W, Haq N, Tahir M, Razaque G. The Impact of Antihypertensive Agents on Health-Related Quality of Life of Hypertensive Patients. Modern Health Science 2021;4:1–7. https://doi.org/10.30560/mhs.v4n1p7.
5. Alshammari S, Alajmi A, Albarrak R, Alaqil A, Alsaeed G, Alzayed M, et al. Quality of Life and Awareness of Hypertension Among Hypertensive Patients in Saudi Arabia. Cureus 2021;13. https://doi.org/10.7759/cureus.14879.
6. Parra D, Romero L, Cala L. Calidad de vida relacionada con la salud en personas con hipertensión y diabetes mellitus. Enfermeria Global 2021;20:331–44. https://doi.org/10.6018/eglobal.423431.
7. Zheng E, Xu J, Xu J, Zeng X, Tan W, Li J, et al. Health-Related Quality of Life and Its Influencing Factors for Elderly Patients With Hypertension: Evidence From Heilongjiang Province, China. Frontiers in Public Health 2021;9:1–8. https://doi.org/10.3389/fpubh.2021.654822.
8. Shah R, Patel J, Shah A, Desai G, Buch J. Determinants of health-related quality of life in patients with hypertension. National Journal of Physiology, Pharmacy and Pharmacology 2020;10:1. https://doi.org/10.5455/njppp.2020.10.02031202011022020.
9. Mohammed A, Mohammad Z, Jetly K, Abd Razak M, Ramli N, Wan W, et al. The Prevalence and Risk Factors of Hypertension among the Urban Population in Southeast Asian Countries: A Systematic Review and Meta-Analysis. International Journal of Hypertension 2021;1:1–14. https://doi.org/10.1155/2021/6657003.
10. Huang K, Chang C, Yu K, Hsu C. Assessment of quality of life and activities of daily living among elderly patients with hypertension and impaired physical mobility in home health care by antihypertensive drugs plus acupuncture A CONSORT-compliant, randomized controlled trial. Medicine (United States) 2022;101:1–8. https://doi.org/10.1097/MD.0000000000029077.
11. Monterrey M, Linares L, Toledo R, Vázquez A, Rivera D, Morales C. Adherencia farmacológica y calidad de vida relacionada con la salud en adultos mayores hipertensos. Revista de Ciencias Médicas de Pinar Del Río 2021;25:1–11.
12. Boima V, Yeboah A, Kretchy I, Koduah A, Agyabeng K, Yorke E. Health-related quality of life and its demographic, clinical and psychosocial determinants among male patients with hypertension in a Ghanaian tertiary hospital. Ghana Medical Journal 2022;56:5–14. https://doi.org/10.4314/gmj.v56i1.2.
13. Gonzalez-Argote J. A Bibliometric Analysis of the Studies in Modeling and Simulation: Insights from Scopus. Gamification and Augmented Reality 2023;1:5–5. https://doi.org/10.56294/gr20235.
14. Rodríguez FAR, Flores LG, Vitón-Castillo AA. Artificial intelligence and machine learning: present and future applications in health sciences. Seminars in Medical Writing and Education 2022;1:9-9. https://doi.org/10.56294/mw20229.
15. Aveiro-Róbalo TR, Pérez-Del-Vallín V. Gamification for well-being: applications for health and fitness. Gamification and Augmented Reality 2023;1:16–16. https://doi.org/10.56294/gr202316.
16. Inastrilla CRA. Data Visualization in the Information Society. Seminars in Medical Writing and Education 2023;2:25-25. https://doi.org/10.56294/mw202325.
17. Barrios CJC, Hereñú MP, Francisco SM. Augmented reality for surgical skills training, update on the topic. Gamification and Augmented Reality 2023;1:8–8. https://doi.org/10.56294/gr20238.
18. Snarska K, Chorąży M, Szczepański M, Wojewódzka M, Ładny J. Quality of life of patients with arterial hypertension. Medicina (Lithuania) 2020;56:1–11. https://doi.org/10.3390/medicina56090459.
19. Amer M, Ur-Rahman N, Rashid S, Jabeen M, Ehsan M. Assessment of blood pressure and health-related quality of life among hypertensive patients: An observational study. Alternative Therapies in Health and Medicine 2019;25:26–31. https://doi.org/10.5414/CP202257.PMID.
20. Malengue A, Morales I. Hipertensión arterial y calidad de la atención en pobladores de aldeas de Angola. Revista Científica de Ciencias de La Salud 2021;14:50–5. https://doi.org/10.17162/rccs.v14i1.1481.
21. Fernández C, Baptista P. Metodología de la Investigación. 2015:634.
22. Corporation RAND. 36-Item Short Form Survey ( SF-36 ) 2019. https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form.html.
23. Ware J. SF-36 Health Survey update. Spine 2000;25:3130–9. https://doi.org/10.1097/00007632-200012150-00008.
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Lucia Asencios-Trujillo, Lida Asencios-Trujillo, Carlos La Rosa-Longobardi, Djamila Gallegos-Espinoza, Livia Piñas-Rivera, Hernan Matta-Solis.
Data curation: Lucia Asencios-Trujillo, Lida Asencios-Trujillo.
Formal analysis: Lida Asencios-Trujillo.
Acquisition of funds: Djamila Gallegos-Espinoza, Livia Piñas-Rivera.
Research: Hernan Matta-Solis, Lucia Asencios-Trujillo, Lida Asencios-Trujillo.
Methodology: Lida Asencios-Trujillo.
Project management: Djamila Gallegos-Espinoza, Livia Piñas-Rivera.
Resources: Lucia Asencios-Trujillo, Lida Asencios-Trujillo.
Software: Lucia Asencios-Trujillo, Lida Asencios-Trujillo.
Supervision: Lucia Asencios-Trujillo, Lida Asencios-Trujillo.
Validation: Lucia Asencios-Trujillo, Lida Asencios-Trujillo, Carlos La Rosa-Longobardi.
Display: Lucia Asencios-Trujillo.
Drafting - original draft: Djamila Gallegos-Espinoza, Livia Piñas-Rivera.
Writing - proofreading and editing: Lucia Asencios-Trujillo.