ORIGINAL BREVE
Quality of Life in Diabetic University professors Treated in Outpatient Clinic for Care in a Hospital in Lima
Calidad de vida en profesores universitarios diabéticos atendidos en consulta externa de atención en un hospital de Lima
Lida Asencios-Trujillo1 ![]() *, Lucia
Asencios-Trujillo1
*, Lucia
Asencios-Trujillo1 ![]() *, Carlos La
Rosa-Longobardi1
*, Carlos La
Rosa-Longobardi1 ![]() *, Djamila
Gallegos-Espinoza1
*, Djamila
Gallegos-Espinoza1 ![]() *, Livia
Piñas-Rivera1
*, Livia
Piñas-Rivera1 ![]() *, Hernan Matta-Solis2
*, Hernan Matta-Solis2
![]() *
*
1Universidad Nacional de Educación Enrique Guzmán y Valle. Escuela de Posgrado. Lima, Perú.
2Instituto Peruano de Salud Familiar. TIC Research Center: eHealth & eEducation. Lima, Perú.
Citar como: Trujillo LA, Asencios-Trujillo L, Rosa-Longobardi CL, Gallegos-Espinoza D, Piñas-Rivera L, Matta-Solis H. Quality of Life in Diabetic University professors Treated in Outpatient Clinic for Care in a Hospital in Lima. Salud, Ciencia y Tecnología 2023; 3:554. https://doi.org/10.56294/saludcyt2023554.
Recibido: 05-06-2023 Revisado: 21-08-2023 Aceptado: 25-10-2023 Publicado: 26-10-2023
Editor: William
Castillo-González ![]()
ABSTRACT
Introduction: the quality of life in diabetics is one of the priorities faced by the health professional for their necessary care, therefore, the research objective is to determine the quality of life in diabetic university professors treated in an outpatient clinic for their care in a hospital in Lima.
Methods: it is a quantitative, descriptive and cross-sectional study, with a population of 113 diabetic participants who answered a questionnaire of sociodemographic aspects and the diabetes 39 instrument for data collection.
Results: in their results, it is observed that 18 (15,9 %) of diabetic university professors have a low quality of life, 77 (59,3 %) mean quality of life and 28 (24,8 %) high quality of life.
Conclusions: it is concluded that university professors with diabetes mellitus should be guided about life changes in university professors with the presence of the disease.
Keywords: Quality of Life; Diabetes Mellitus; Public Health; Noncommunicable Diseases.
RESUMEN
Introducción: la calidad de vida en diabéticos es una de las prioridades que enfrenta el profesional de la salud para su necesaria atención, por lo tanto, el objetivo de la investigación es determinar la calidad de vida en profesores universitarios diabéticos atendidos en consulta externa para su atención en un hospital de Lima.
Métodos: es un estudio cuantitativo, descriptivo y transversal, con una población de 113 participantes diabéticos que respondieron un cuestionario de aspectos sociodemográficos y el instrumento diabetes 39 para la recolección de datos.
Resultados: en sus resultados se observa que 18 (15,9 %) de los profesores universitarios diabéticos tienen una calidad de vida baja, 77 (59,3 %) calidad de vida media y 28 (24,8 %) calidad de vida alta.
Conclusiones: se concluye que se debe orientar a los profesores universitarios con diabetes mellitus sobre los cambios de vida en los profesores universitarios con presencia de la enfermedad.
Palabras clave: Calidad de Vida; Diabetes Mellitus; Salud Pública; Enfermedades no Transmisibles.
INTRODUCTION
The World Health Organization (WHO) estimates that Type II Diabetes Mellitus (T2DM) is the third highest risk factor for premature mortality worldwide, preceded only by high blood pressure and tobacco. In addition, extensive epidemiological studies show that the incidence of T2DM is increasing worldwide.(1) It affects 463 million university professors, and the overall figure is projected to rise to 629 million by 2045 and represents approximately 90 % of all patients with diabetes.(2,3)
Diabetes currently affects more than 425 million university professors worldwide, and is projected to rise to 642 million university professors by 2040, which is 50 % more than current records; As a consequence, complications from diabetes will also increase.(4)
Diabetes mellitus is associated with approximately 4,6 million deaths per year and is among the top 10 causes of decline in the productive capacity of individuals worldwide.(5,6)
It is one of the most common preventable chronic diseases worldwide that is associated with abnormal blood sugar levels.(7) This may be due to inadequate insulin production in the body or because cells are no longer sensitive to perform their actions.(8,9)
Management of T2DM focuses primarily on monitoring blood glucose levels, taking medications, and educating patients to maintain behaviors, which is critical to achieving good clinical outcomes and quality of life.(10,11,12)
It generates various complications. In relation to functional disability, it can be multifactorial, however, ophthalmopathy, nephropathy, neuropathy and coronary artery disease are the most disabling according to the determined group. Quality of life is reduced by the limitation of physical activities of all kinds.(13)
Quality of life is a phenomenon that brings about transformations in society and "considers factors related to university professors’ health, changes in family structure and population growth of older adults".(14,15)
In a study conducted in India,(16) evidence has shown that medical nutrition therapy (NTM) is a valuable approach and an essential component of Prevention and Management of T2DM. Studies have shown that nutrition for high-fiber diabetes (FDN) has multisystem health benefits, including improved glycemic control, reduced glucose spikes, decreased hyperinsulinemia, improved plasma lipid concentrations, and weight management in patients with T2DM.
In a study conducted in Ecuador(17), 57 mainly female participants met the inclusion and exclusion criteria, with a mean age of 67,77 years. The most frequent health status was 11111 (28,1 %) which means "no discomfort".
In a study conducted in Peru(18), 50,60 % (n = 80) of the participants were women. The mean age was 63,5 ± 12,10 years. The most representative family figure of primary caregiver was the child in 50,6 % (n = 80) followed by the spouse 20,3 % (n = 32). Of the 158 subjects, 98 (62 %) had controlled glycemic control and of these 44 (44,9 %) adequate families’ supports. Of the 60 unchecked, 16 (26,6 %) had adequate family support. The association between family support and glycemic control was determined being statistically significant X2=5,252, with a ρ<0,05.
Therefore, the objective is to determine the quality of life in diabetic university professors treated in outpatient care in a hospital in Lima.
While it is true to investigate or inquire about the quality of life in diabetic university professors, it presents a very significant justification at the health and education level; Given that, diabetes being a chronic disease affects various physical, emotional and social aspects, so, you have to understand this condition and how it affects teachers, since this research will provide valuable information in which, you can inform about the challenges they face in their lives, in teaching and in the general health of university professors.
METHODS
Research type and Design
In the present research according to its properties is quantitative, descriptive-transverse and non-experimental methodology.(19)
Population and Sample
The total population is made up of 113 patients who perform their care in a hospital in Lima. According to the bias of the voluntary response sample, it was carried out in a census manner for data collection since our type of sampling in our study was for convenience.
Inclusion Criteria
• Participants over 30 years old
• Participants who are seen in the hospital's endocrinology service
• Participants who voluntarily agree to participate in the study.
• Participants who signed the inform consent CIE IPSF 029-2023. It was previously accepted by the institution.
Exclusion Criteria
• Participants under 30 years old
• Non-endocrinology participants
• Participants who do not sign the informed consent.
Technique and Instrument
The technique for data collection was the survey, in which sociodemographic aspects and the Diabetes 39 data collection instrument are found.
The data collection instrument Diabetes 39 comprises 39 items distributed in 5 dimensions: energy and mobility (15 items), diabetes control (12 items), control and worry (4 items), social overload (5 items) and sexual function (3 items), in which it is valued with a Likert-type scale with 7 response options: "1 = not affected at all", "2 = almost nothing", "3 = a little", "4 = fair", "5 = a lot", "6 = too much", "7 = tremendously affected", so its score would be "1 to 91" is low quality of life, "92 to 183" half-life quality and "184 to 273" high quality of life, the higher the score, the higher the patient's quality of life".(20,21)
The validity of the instrument was determined based on the exploratory factor analysis technique with the Kaiser-Mayer-Olkin sample adequacy measure, obtaining a coefficient of 0,950 (KMO> 0,6), while Bartlett's sphericity test obtained results significant (X2 approx. = 9497,371; gl = 742; p = 0,000).
The reliability of the instrument was determined based on the Cronbach's Alpha statistical test, a coefficient of 0,994 (α> 0,8).
The results of the validity and reliability tests carried out to date attest to the relevance of the 39-item questionnaire (Diabetes-39) as a valid discriminative instrument, which shows significant correlations with a general assessment of quality of life, the pattern of diabetes, severity and comorbidity.(20)
Place and Application of the Instrument
For the research, prior coordination was made with the head doctor of the endocrinology consultation area for the realization of the study, in turn, previous details about what will be done in the research and thus have the necessary knowledge. A follow-up prior to the completion of the survey in the months of March to April of this year.
RESULTS
In Figure 1, it can be seen that 15,9 % (n=18) of the participants have a low quality of life, 59,3 % (n=77) a median quality of life and 24,8 %(n=28) a high quality of life.
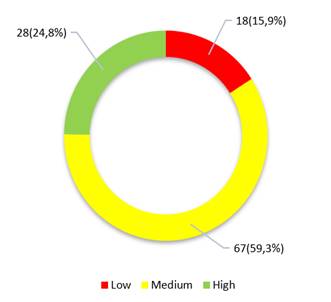
Figure 1. Quality of life in diabetic university professors treated in outpatient clinics for their care in a hospital in Lima
In Figure 2, it can be observed with respect to their dimensions of quality of life, where, in the energy-mobility dimension, 21,2 % (n = 24) of the participants have a low quality of life, 68,1 % (n = 77) a mean quality of life and 10,6 % (n = 12) a high quality of life, in terms of the diabetes control dimension, 20,4 % (n=23) participants have a low quality of life, 56,6 % (n=64) a median quality of life and 23 % (n=26) a high quality of life, in the anxiety-worry dimension, 23 % (n=26) of the participants have a low quality of life, 53,1 % (n=60) a median quality of life and 23,9 %(n=27) a high quality of life, In the social burden dimension, 24,8 % (n=28) of the participants have a low quality of life, 54 % (n=61) a mean quality of life and 21,2 %(n=24) a high quality of life; and in the dimension sexual functioning, 32,7 % (n=37) of the participants had a low quality of life, 56,6 % (n=64) a median quality of life and 10,6 %(n=12) a high quality of life.
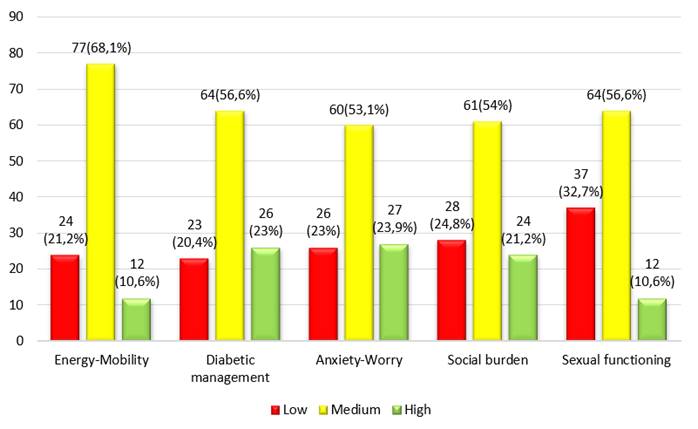
Figure 2. Quality of life in relation to its dimensions in diabetic university professors treated in outpatient care in a hospital in Lima
In Figure 3, the sex of the participants can be observed in relation to their quality of life, where, the male sex, 50 % (n=14) had a high quality of life, 61,2 % (n=41) a mean quality of life and 16,7 % (n=3) a low quality of life; and with respect to the female sex, 50 % (n=14) had a high quality of life, 38,8 % (n=26) had a median quality of life and 83,3 % (n=15) had a low quality of life.
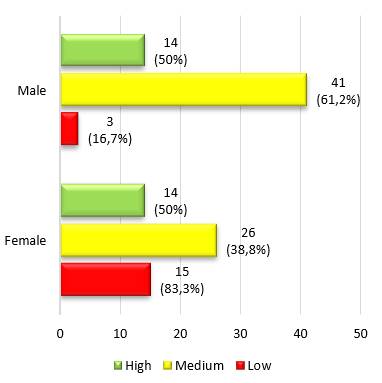
Figure 3. Quality of life in relation to sex in diabetics treated in outpatient care in a hospital in Lima
In Figure 4, we can observe the age of the participants and their relationship with quality of life, where, participants between the ages of 30 to 59 years, 10,7 % (n = 3) have a high quality of life, 43,3 % (n = 29) have a mean quality of life and 72,2 % (n = 13) have a low quality of life and participants between ages and 60 to 80 years, 89,3 % (n=25) have a high quality of life, 56,7 % (n=38) have a median quality of life and 27,8 % (n=5) have a low quality of life.

Figure 4. Quality of life in relation to the age of diabetics treated in outpatient care in a hospital in Lima
DISCUSSION
In the present research, it was given from the perspective of cardiovascular and metabolic health, where the promotion and prevention in diabetic university professors to improve their quality of life.
In the results of the main variable quality of life, we observe that most of the diabetic university professors in the study have a median quality of life, we can interpret that diabetic university professors at the time of being diagnosed with the disease, do not adequately perform the recommendations provided by health professionals, since their quality of life is even more compromised. Since factors such as being overweight and obsessive, age, not performing physical activity and not presenting an adequate diet, causes the quality of life in the diabetic person to decrease.(18,20)
Regarding the results of quality of life in relation to their dimensions, we observed that most of them developed a half-life quality, this is because diabetic university professors have considerable problems in mobility affecting the peripheral nerves, generating pain in the person and even causing problems in organs such as the heart and bladder; In addition, diabetics are likely to suffer mental disorders such as anxiety and depression at considerable levels, since, when they have a chronic illness, the consumption of medication daily and not performing their routines before the disease, causes their mental health to be also compromised. Therefore, family support will be very important for the diabetic person to cope with the disease, and to be able to properly follow their treatment and maintain their stable mental health.(21)
In the results of quality of life according to the ages, we observe that in the ages of 60 to 80 years tend to present a better quality of life, this is because diabetes mellitus appears more in young university professors, because the ease of carrying high glucose index in the blood, because young university professors are less aware of the disease, where the phacotres of an inadequate diet, the consumption of alcohol, sedentary lifestyle and obesity, are factors that can lead to the disease, so you can go throughout your life with this disease. Abuhadba et al.(18) mention that being younger, the risks of presenting diabetes mellitus increase, this is because the excessive consumption of fat, sugars and carbohydrates, increases the chances of presenting metabolic and cardiovascular diseases, and that the majority is usually related to overweight and obesity, arterial hypertension and high cholesterol, initiating a phase of diabetes mellitus.(22)
Regarding the results of quality of life in relation to age we observe that most university professors have an average quality of life, this can be interpreted in that, age as it progresses in diabetic university professors, their quality of life begins to reduce, because being vulnerable to different diseases, Diabetes eventually damages the heart, blood vessels, eyes, kidneys, and nerves. Therefore, many adults and older adults tend to have an increased risk of problems such as myocardial infarctions and strokes, foot ulcers and infection, blindness due to damage to the capillaries of the retina as time progresses, kidney failure, erectile dysfunction in men, hearing problems, sleep apnea, and risk of suffering from Alzheimer's, so improving the quality of life of diabetics, will reduce these types of risks that the disease can cause and thus can extend their lives if they make healthy habits to postpone their years of life.
The research will be beneficial for future studies since the quality of life in diabetic patients is an issue of great importance today, given that this disease is manifesting more regularly in younger university professors as shown years ago, so when conducting this study, it should be taken into account that healthy habits can be made to improve quality.
This research work will be beneficial for future studies, since the study focused on the quality of life of university professors with diabetes, whose importance is that it will allow to know how they chose to develop skills or abilities that allowed them to maintain their healthy quality of life, given that, the quality of life in them is a constant change, Since presenting a chronic disease where their physical, emotional and social state have to stay balanced so that their quality of life does not decrease, in addition to having family support is a positive factor for themselves.
CONCLUSIONS
It is concluded that, it is due to educate the young population about healthy habits to take into account that allow to improve their quality of life and thus avoid developing any disease. It is concluded that, itis necessary to guide university professors with diabetes mellitus on life changes in university professors with the presence of the disease. It is concluded that home visits should be made to diabetic patients, to educate the person and their families, about food and self-care.
BIBLIOGRAPHIC REFERENCES
1. Baroni I, et al. Self-care and type 2 diabetes mellitus (T2DM): a literature review in sex-related differences. Acta Biomed. 2022;93(4). doi: 10.23750/abm.v93i4.13324.
2. Ikegami H, Hiromine Y, Noso S. Insulin-dependent diabetes mellitus in older adults: Current status and future prospects. Geriatr Gerontol Int. 2022;22(8):549–53. doi: 10.1111/ggi.14414.
3. McMorrow R, Hunter B, Hendrieckx C, et al. Assessing and addressing diabetes distress among adults with type 2 diabetes: An online survey of Australian general practitioners. Prim Care Diabetes. 2022;16(5):692–7. doi: 10.1016/j.pcd.2022.08.001.
4. Sánchez K, Monroy J, Jaimes J, et al. Risk factors associated with diabetic neuropathy in Mexican patients. Cir Cir. 2021;89(2):189–99. doi: 10.24875/CIRU.20000243.
5. Rafael V, Medranda A, Ayala E. Quality of sexual life in patients with type 2 diabetes mellitus in an Ecuadorian province. Rev Eugenio Espejo. 2022;16(3):26–36. doi: 10.37135/ee.04.15.04.
6. Navarro E, Tarraga M, Marcos F, et al. Prevention of amputations related to diabetic foot. J Negat not Posit results. 2022;7(2):235–65. doi: 10.19230/jonnpr.4450.
7. Ali A, Alfajjam S, Gasana J. Diabetes Mellitus and Its Risk Factors among Migrant Workers in Kuwait. Int J Environ Res Public Health. 2022;19(7). doi: 10.3390/ijerph19073943.
8. Thipsawat S. Early detection of diabetic nephropathy in patient with type 2 diabetes mellitus: A review of the literature. Diabetes Vasc Dis Beef. 2021;18(6):1–9. doi: 10.1177/14791641211058856.
9. Tornese G, Schiaffini R, Mozzillo E, et al. The effect of the COVID-19 pandemic on telemedicine in pediatric diabetes centers in Italy: Results from a longitudinal survey. Diabetes Res Clin Practice. 2021;179:109030. doi: 10.1016/j.diabres.2021.109030.
10. Das A, et al. Health care delivery model in India with relevance to diabetes care. Heliyon. 2022;8(10):e10904. doi: 10.1016/j.heliyon.2022.e10904.
11. Cousin E, et al. Diabetes mortality and trends before 25 years of age: an analysis of the Global Burden of Disease Study 2019. Lancet Diabetes Endocrinol. 2022;10(3):177–92. doi: 10.1016/S2213-8587(21)00349-1.
12. Harris S, et al. Association of statin and/or renin-angiotensin-aldosterone system modulating therapy with mortality in adults with diabetes admitted to hospital with COVID-19: A retrospective multicentre European study. Diabetes Metab Syndr Clin Res Rev. 2022;16(5). doi: 10.1016/j.dsx.2022.102484.
13. Ibáñez E, et al. Frequency of chronic complications in patients with type 2 diabetes mellitus in a third level hospital. Rev Virtual Soc Paraguaya Med Interna. 2022;9(1):45–54. https://doi.org/10.18004/rvspmi/2312-3893/2022.09.01.45.
14. Lara J, Garcia H. Quality of life and self-esteem in older adults of an association of Ecuadorian retirees. Chakiñan. 2022;17(1):95–108.
15. Randy S, Cuzquen D, Marie R, Huamanchumo E. Quality of life at work of the municipal collaborators of Túcume – Peru. 2022.
16. Saboo B, et al. Role and importance of high fiber in diabetes management in India. Diabetes Metab Syndr Clin Res Rev. 2022;16(5):102480. doi: 10.1016/j.dsx.2022.102480.
17. Rojas G, Solís P, Gaona R, et al. Quality of life in a group of patients with type 2 diabetes mellitus: a cross-sectional study. Rev medica Vozandes. 2021;32(1):13–22. doi: 10.48018/rmv.v32.i1.7.
18. Abuhadba C, Spirit N, Gamarra D. Association between family support and glycemic control in patients with type 2 diabetes mellitus in an Endocrinology Clinic of a national hospital. Horiz Physician. 2021;21(4):e1489. https://doi.org/10.24265/horizmed.2021.v21n4.07.
19. Téllez FC, Gimenez M, González C. Education for the control of arterial hypertension in older adults: An effective approach. Community and Interculturality in Dialogue 2021;1:3-3. https://doi.org/10.56294/cid20213.
20. Boyer J, Earp J. The Development of an Instrument for Assessing the Quality of Life of University professors with Diabetes: Diabetes-39. Med Care. 1997;35(5):440–53. https://doi.org/10.1097/00005650-199705000-00003.
21. Rodríguez P, Mamani B. Educational intervention in diabetic older adults of Jujuy. Community and Interculturality in Dialogue 2021;1:2-2. https://doi.org/10.56294/cid20212.
22. López J, Rodriguez R. Adaptation and validation of the Diabetes 39 quality of life instrument in Mexican patients with type 2 diabetes mellitus. Salud Publica de Mexico. 2006; 48(3):200–11.
FINANCING
The authors did not receive financing for the development of this research.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Lucia Asencios-Trujillo, Lida Asencios-Trujillo, Carlos La Rosa-Longobardi, Djamila Gallegos-Espinoza, Livia Piñas-Rivera, Hernan Matta-Solis.
Data curation: Lucia Asencios-Trujillo, Lida Asencios-Trujillo
Formal analysis: Lida Asencios-Trujillo
Acquisition of funds: Djamila Gallegos-Espinoza, Livia Piñas-Rivera
Research: Hernan Matta-Solis, Lucia Asencios-Trujillo, Lida Asencios-Trujillo
Methodology: Lida Asencios-Trujillo
Project management: Djamila Gallegos-Espinoza, Livia Piñas-Rivera
Resources: Lucia Asencios-Trujillo, Lida Asencios-Trujillo
Software: Lucia Asencios-Trujillo, Lida Asencios-Trujillo
Supervision: Lucia Asencios-Trujillo, Lida Asencios-Trujillo
Validation: Lucia Asencios-Trujillo, Lida Asencios-Trujillo, Carlos La Rosa-Longobardi
Display: Lucia Asencios-Trujillo
Drafting - original draft: Djamila Gallegos-Espinoza, Livia Piñas-Rivera
Writing - proofreading and editing: Lucia Asencios-Trujillo